The OneLondon Citizens’ Summit brought together 100 Londoners to debate and deliberate some of the complex issues around uses of health and care data. Held in February and March 2020, the Summit identified Londoners’ expectations as to: how their health and care data should be used, who should have access to it, and for what purpose. These expectations were delivered as recommendations to a panel of local and national system leaders, politicians and policymakers.
The OneLondon Citizens’ Summit is an example of deliberative public engagement: a unique approach which empowered Londoners to have their say and to inform policy and practice in a way that builds legitimacy and trust.
Here you will find all of the materials and stimulus used over the four days of the Citizens’ Summit. This includes slide decks, handouts and videos of expert presentations.
A full report setting out the recommendations and conditions formed by participants at the Summit is available here.
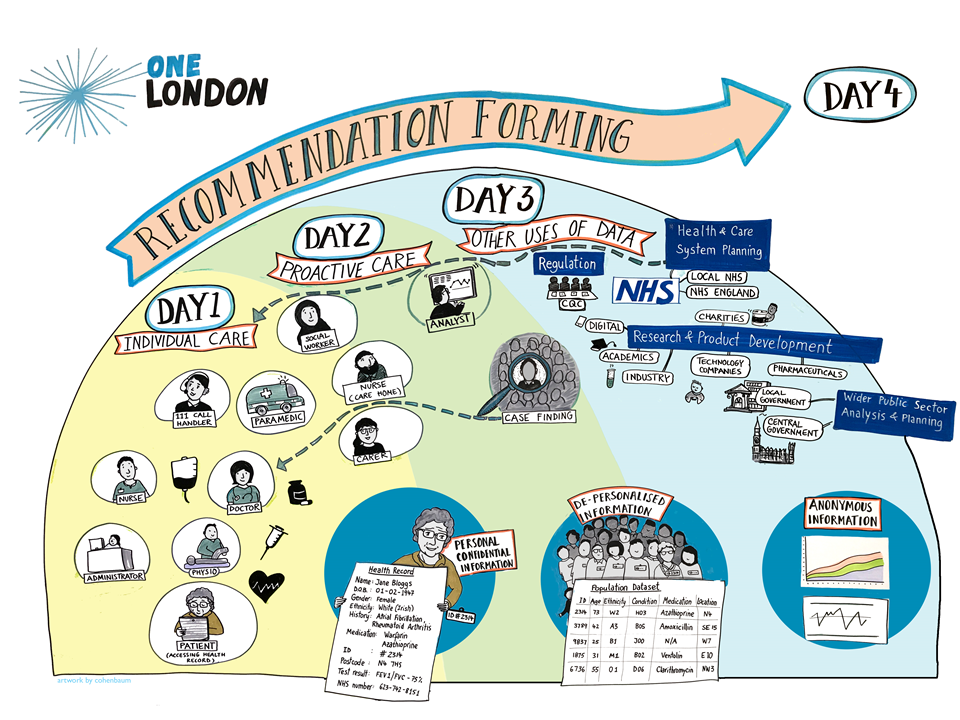
The Citizens’ Summit was held over four days with the same 100 participants – reflective of the diverse population of London.
Day 1 focused on use of data for individual care in a health setting, including access and control
Day 2 looked at use of data for individual care in a social care setting, including access and control; and the use of de-personalised data for proactive care
Day 3 considered issues around the approval of requests to access data for ‘secondary uses’ (including planning, improvement and research) based on Londoner’s thoughts on what constitutes ‘public benefit’
Day 4 comprised recommendation forming based on the first three days, including issues around ongoing public involvement in the oversight in the use of data for planning and research
Day 1
Day 1 focused on use of data for individual care in a health setting, including access and control.
Introduction
Professor Michael Burgess, Chair in Biomedical Ethics at the University of British Columbia and Independent Academic Advisor for the OneLondon Citizens’ Summit, introduces the four-day deliberative process, including ground rules.
Mark Kewley, Programme Director for OneLondon, introduces the OneLondon Local Health and Care Record Exemplar (LHCRE), highlighting why the process of deliberative public engagement has been chosen.
A video from The Mayor of London, endorsing the OneLondon Citizens’ Summit, highlights the importance of this process and of Londoners’ having their say as to how their health and care data is used.
Expectations of health and care services
Dan Wellings, Senior Fellow in The King’s Fund Policy Team provides an introduction to the NHS and social care, highlighting the range of organisations involved. Introducing patient data flow diagrams, Dan explains that a care team is made up of a whole host of individuals.
Participant tables reflect on what they’ve just heard, prompted by questions from facilitators:
How familiar were you with the way the NHS and social care is run and organised nowadays; was there anything in that presentation that was new or surprising to you; does it leave you with any questions or concerns?
What is health and care data and how can it be used?
Spontaneous discussion at tables, prompted by questions from facilitators.
What health and care information do you think is held about you, why and by whom; how joined up do you think health and care services are when it comes to using information; how joined up do you think health and care services should be?
Video produced by the Professional Records Standards Body and Understanding Patient Data shows some of the ways that data is used in the NHS and social care.
What is health and care data, and how can it be used? Murat Soncul, former Information Governance Lead for OneLondon, provides an overview.
Expert lightning talk: Paramedic and Chief Clinical Information Officer of London Ambulance Service, Stuart Crichton, provides his perspective as a first responder.
Expert lightning talk: Dr Axel Heitmueller from Imperial College Health Partners explores the uses of data for proactive care and its role in research.
In his second presentation of Day 1, Information Governance expert Murat Soncul highlights the rules and regulations in place around the uses of health and care data.
Table discussions followed Murat’s second presentation as participants reflected on what they had just heard, what interested them most, what they found concerning, and any opportunities or risks associated with using data in some of the ways described. This was followed by a Q&A with the expert panel.
Access and control: providing care to an individual
This session focussed on the entire healthcare team (in a health setting), and who has access to what information. Participants considered the following: when you think of the entire healthcare team, who do you think of; who do you think has access to your health data or records; what kinds of information do you think they can access and why?
Mark Kewley provides an overview of who has access to what information in a health setting, and describes the aspects of a control environment (legal frameworks, employment and professional conditions, personal and technological controls). He describes how this plays out in a world of predominantly paper records, along with technical and feasibility constraints.
Dr Sanjay Gautama, Consultant Anaesthetist at Imperial College Healthcare NHS Trust, explains who makes up a care team and explains the complexity of the issue around access for participants to consider, including: privacy, convenience (for patients and staff), safety, and burden on the NHS.
Using handouts and case studies as stimulus, participants consider who should have access to what information in a health setting, deliberating trade-offs around privacy, convenience, patient safety, burden on staff, and efficiency. They then rank case studies in order of most to least comfortable.
Facilitators report back to the room on table discussions: agreed and proposed categories for roles based access, difficult decisons they had to make, what was important to them in deciding whether or not to give different roles access to information.
Assessment and temperature check: where the room is at, is there divergence (and why), and what is important to people in terms of the trade-offs around roles based access.
Day 2
Day 2 looked at use of data for individual care in a social care setting, including access and control; and the use of de-personalised data for proactive care.
Introduction
Chair welcomes participants back and summarises what happened on Day 1. Provides a reminder of the ground rules and for people to continue to think in a civic-minded way, before giving an overview of the topics to be discussed today.
Access and control: providing care to an individual
Cathy Ingram from the Integrated Care Transformation Team at Guy’s & St Thomas’ NHS Trust describes some of the main care settings and the information that’s relevant in each. She explains what information these settings tend to receive from the health system and why this is.
Jonty Heaversedge, OneLondon Clinical Lead and a GP in South East London introduces the idea of standardising access to certain information for different roles to facilitate faster, safer care. He introduces the trade-offs for participants to consider, using examples such as a care plan versus a hospital discharge summary.
Case studies help participants to consider who should have access to what information in a social care setting, deliberating the various trade-offs. After ranking the case studies in order of most to least comfortable, tables discuss categories of role access for social care.
Tables report back to the room, focusing on the reasons underpinning decisions about who should see what social care data, and drawing out any differences between NHS and social care. Chair assesses the temperature of the room, summarising any divergence.
Access and control: proactive care
Jonty Heaversedge provides an overview of what proactive care is, with examples, and explains how technology and joined-up information is enabling this. He highlights some of the benefits and some of the concerns. Tables have chance to reflect on this.
Health Economist, Andi Orlowski, introduces the kinds of people involved in proactive care, and the types of controls that are in place. Tables reflect on this, with opportunity for Q&A. Following this, OneLondon’s Mark Kewley provides additional context, drawing out some of the additional concerns around using data for proactive care.
Case studies enable participants to consider different examples of proactive care, highlighting that this uses de-personalised data. Participants consider the acceptability of using data for proactive care, deliberating the reassurances that need to be in place for Londoners to be comfortable with this.
Tables report back to the room, summarising their discussions in relation to proactive care, specifically the levels of acceptability, reassurances that need to be in place, and whether it’s acceptable to continue to deliver proactive care under the implied consent model. Participants vote and are asked if they’d like to make a recommendation.
Wrap-up of first weekend
Mark Kewley reflects on the first weekend of the Citizens’ Summit, giving an overview of the journey to date and what’s to come in the second weekend.
Day 3
Day 3 considered issues around the approval of requests to access data for ‘secondary uses’ (including planning, improvement and research) based on Londoners’ thoughts on what constitutes ‘public benefit’.
Introduction
Chair summarises the story so far, including what was covered on days 1 and 2. and where we are going in days 3 and 4 – moving away from uses of data for individual care, to secondary uses including planning, improvement, research and innovation.
Use of de-personalised data for health and care planning and improvement: the diameter of trust
Mark Kewley provides further explanation of de-personalised data. He highlights that all data uses referred to in day 3 would use this type of data or data that’s completely anonymous. He poses the question: what would make the use of this kind of data for different purposes more or less trustworthy?
Alex Baylis, Assistant Director of Policy at The King’s Fund, describes how planning and improvement happens across health, social care, and public health.
Tables reflect on what they’ve heard: including anything that was new or surprising to them. There’s then chance to quiz a panel of experts about this type of data use, including Alex Baylis, The King’s Fund; Dr Jonty Heaversedge, GP; and Luke Readman, Chief Officer for OneLondon.
Tables consider case studies that use de-personalised data for planning and improvement. They discuss whether they’d expect providers to be using data in this way; whether this is a legitimate use of data; and which organisations they’re comfortable with being involved.
Tables report back to the room. Chair provides reassurance that we’ll revisit this discussion on day 4 before moving to make a recommendation on data use for planning and improvement.
Use of de-personalised data for research and innovation
Caroline Cake, CEO of Health Data Research UK explains what research and development is, who does it, why it’s important, and the benefits and risks. She highlights why linked data offers a new type of opportunity.
Amanda Lucas, Lead for the Discover-NOW Health Data Research Hub, explains the legal basis for using data for research and introduces the concept of the ‘five safes’.
Tables consider practicalities of how different people involved in research can access the data in a trustworthy way. Using case studies, they consider examples of de-personalised data being used for research and development, and deliberate what might increase trustworthiness for each.
Use of de-personalised data for research and development
Axel Heitmueller, MD of Imperial College Health Partners explains the value of health data, the cost of maintaining and curating this data, and some of the partnership models that are in play – highlighting the benefits and concerns.
Tables reflect on what they’ve heard, and if anything is unclear or confusing. Facilitators tease out potential questions for the follow-up panel of representatives from organisations focused on using NHS data for research and development.
Academic researcher Tim Hubbard, explains how and why partnerships are formed with the NHS to support academic research.
Harpreet Sood, a primary care doctor at University College London Hospitals, shares an NHS Trust perspective on some of the elements of a fair partnership.
Amy Darlington, Engagement Lead for OneLondon introduces the actors in a fair and productive partnership, and elements such as benefits, costs, income and conditions. She explains that we need participants’ help with setting the conditions of these partnerships.
Tables reflect on what these conditions mean, including income and charging, level of transparency and distribution of benefits. Working through different ‘data request proposals’, participants judge whether the requests should be approved, based on what is a fair deal for the NHS and the party requesting access, considering trade-offs within the various conditions.
Tables report back to the room on their discussions. Chair addresses where there is convergence and divergence, and why, and assesses the temperature of the room in terms of what’s important to people. The session closes with a summary of key considerations that would need to be in place to maintain public trust from what we have just heard. This discussion will be picked up on day 4 as part of the recommendation forming.
Day 4
Day 4 comprised recommendation forming based on the first three days, including issues around ongoing public involvement in the oversight of use of data for planning and research.
Chair explains the purpose of day 4, recapping what has been discussed over days 1 – 3. Participants are split into four working groups, and each group is tasked with forming recommendations around a specific issue. Groups are supported by relevant stimulus and subject matter experts.
Recommendation forming: round 1
Within their working groups, participants are split into two sub-groups to consider the stimulus and draft their recommendations. After an hour, the two sub-groups come back together. They present their recommendations to eachother, and vote on which version they like – or agree to develop a new recommendation from the existing ones. This draft recommendation is written up, ready to be presented back to the summit.
Stimulus for this working group: summary of top-level issues and findings from days 1 and 2; a proposed RBAC model; accompanying data capture to show visually what access might look like in reality for social care; and participant questions (via post-it notes from the ‘graffiti wall’).
Stimulus for this working group: summary of top-level issues and findings from day 3; case studies to return to; and participant questions (via post-it notes from the ‘graffiti wall’).
Stimulus for this working group: summary of top-level issues and findings from day 3; and participant questions (via post-it notes from the ‘graffiti wall’).
Stimulus for this working group: summary of top-level issues and findings from days 1, 2 and 3; examples of how oversight could/has worked for similar/previous pieces of work; parameters of feasibility; and participant questions (via post-it notes from the ‘graffiti wall’).
Presentation of recommendations: round 1
Nominated participants, or facilitators, present their working groups’ recommendation and conditions back to the summit. After each presentation, the room is asked to vote on the level of support for each recommendation. Participants note their comments and feedback on post-it notes for each working group to take back and consider.
Recommendation forming: round 2
Working groups come back together to reflect and consider all comments and questions from summit participants. Supported by facilitators, they work together to reach a final recommendation. This might include changing the wording of the recommendation all together, tweaking it, and/or adding or removing operating principles, conditions, assurances or caveats.
Once the group is happy with their recommendation, the facilitator initiates an open vote, after which follows further discussion to enable the working group the opportunity to tweak the recommendation further. This final recommendation is then presented back to the summit.
Presentation of recommendations: round 2
Nominated participants, or facilitators, present their working groups’ final recommendation and conditions back to the summit.
Consistency across London
Over the course of the summit, participants have heard that for data to be useful for proactive care, planning and research, it relies on data sets being as complete as possible – i.e. containing the data of everyone, not just of certain people or from certain areas of London. As data controllers, GPs and other health and care services, have an important role to play in this. Participants reflect on the range of contrasting views around joining up data for reasons beyond individual care, and consider how policy should be shaped to support this.
An assembled panel of London’s health and care leaders, politicians and policymakers are invited to respond to the recommendations and conditions formed by summit participants. This is followed by a Q&A chaired by Ipsos MORI Chief Executive, Ben Page.
Wrap-up of final weekend
OneLondon’s Mark Kewley wraps up the final weekend of the Citizens’ Summit, reflecting on the four days of deliberation. In thanking participants, experts, and all involved, he sets out next steps and how OneLondon will take the recommendations forward.
OneLondon wishes to thank all participants, facilitators and experts involved in the Citizens’ Summit.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept All”, you consent to the use of ALL the cookies. However, you may visit "Cookie Settings" to provide a controlled consent.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.